
Cleft Lip and Palate
Introduction
A cleft lip is a congenital deformity due to the abnormal discontinuity of lip musculature, lip mucus membrane and skin. It usually occurs in the upper lip.
A cleft palate is a congenital deformity due to an abnormal discontinuity in the palatal musculature, mucus membrane with or without involving a hard palate. It may extend from the uvula to the alveolus.
Etiology
Cleft lip and palate is a multifactorial disease.
It can be syndromic clefts and non-syndromic clefts.
Non-syndromic cleft - etiology:
Genetic predisposition: TGF-alpha, MSX 1, RAR-a, DLX-2, BCL-3
Nutritional disturbances during development
Any physiological or traumatic stress during development
Defective vascular supply to the affected area during development
Mechanical disturbances during development
Effect of certain drugs taken by the mother during development
Alcoholism, smoking during pregnancy
Effect of radiation
Maternal infection
Lack of inherent developmental force
Syndromes associated with cleft lip and palate:
Mendelian disorders:
Van der Woude syndrome
Gorlin syndrome
Treacher Collins syndrome
Orofacial digital syndrome
Stickler syndrome
Oto palato digital syndrome
Non-Mendelian syndrome:
Pierre Robin syndrome
Goldenhar syndrome
Chromosomal aberrations:
Trisomy 13
Trisomy 18
Velocardiofacial syndrome
Teratogens:
Foetal alcohol syndrome
Foetal phenytoin syndrome
Others:
De Lange syndrome
Prevalence
A cleft lip is the most common congenital deformity in the face. WHO report of the International Collaborative Research on Craniofacial Anomalies (2001) said that a child is born with a cleft in the world approximately every 2 1/2 minutes. It is most prevalent in the African population and less prevalent in the Caucasian and Filipino populations.
In India, the incidence of 1.09 in 1000 live births.
Development of Lips and Palate
Upper Lip: The lateral part is formed by the maxillary process. The medial part is formed by the (frontonasal) median nasal process as mesoderm over which the maxillary process grows.
Lower lip: Fusion of left and right mandibular process.
Palate: Premaxilla or the primitive palate formed from the frontonasal process. In the 6th week of intrauterine life, the maxillary process grows horizontally giving the palatal process. As the tongue descends, the right and left palatal processes fuse with each other and also with the primitive palate by the 10th week of IU life.
The cleft lip results from the failure of fusion of the median nasal process with the maxillary process during the 4th to 6th week of IU life. The cleft palate results from the failure of fusion of the right and left palatal processes and/or premaxilla during the 8th to 12th week of IU life.
Classification of Cleft lip and palate
Veau classification:
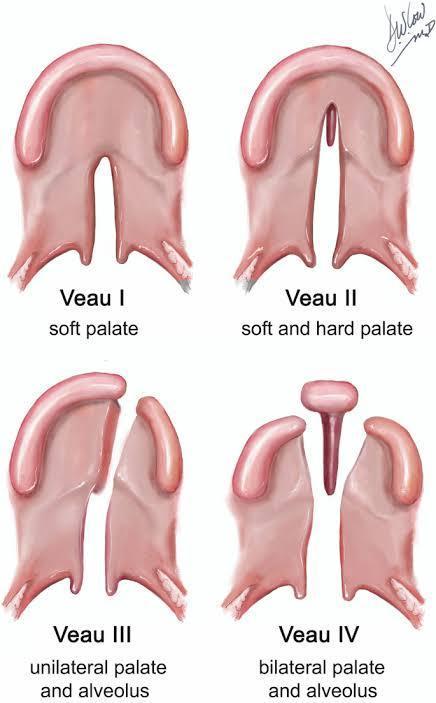
Group 1 - cleft of soft palate only
Group 2 - Cleft involving hard and soft palate only till the incisive foramen (cleft of secondary palate)
Group 3 - Complete unilateral cleft (involving uvula till incisive foramen then deviating one side till the alveolus)
Group 4 - Complete bilateral cleft
Striped Y or Kernahan Classification:
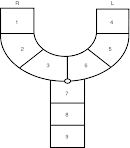
It provides a graphic demonstration of the extent of the cleft.
1 right lip
2 right alveolus
3 right alveolus till incisive foramen
4 left lip
5 left alveolus
6 left alveolus till incisive foramen
7 hard palate
8 hard palate
9 soft palate
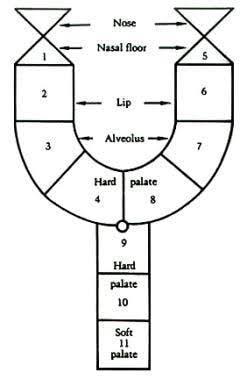
Elsahy modification of Kernahan classification:
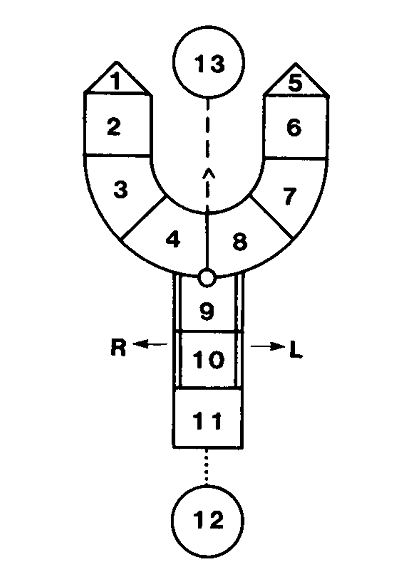
1 right nostril floor
2 right lip
3 right alveolus
4 hard palate anterior to the incisive foramen on right
5 left nostril floor
6 left lip
7 left alveolus
8 hard palate anterior to the incisive foramen on left
9 hard palate
10 hard palate
11 soft palate
12 posterior pharyngeal wall
13 premaxilla
Millard classification (1977):
He added inverted triangles on top of upright triangular segments 1 and 5 for the right and left aspects of the nasal arch.
Features
Feeding problem:
To suckle milk, infants need to create an airtight seal around the nipple with lips and exert negative pressure to express milk. Cleft lip children are unable to exert this pressure due to the discontinuity.
There is communication between nose and mouth in the cleft palate patients. It causes regurgitation of fluids into the nose leading to respiratory problems. Children's feeding posture should be upright to prevent regurgitation.
Speech:
Velopharyngeal incompetence causes hypernasality.
Oronasal fistula causes nasal twang.
Malocclusion causes pronunciation problems.
Recurrent middle ear infections:
Due to the malposition of the eustachian tube.
Malocclusion:
Missing laterals
Impacted canines
Maxillary arch collapse
Narrow maxillary arch
Maxillary growth retardation
Severe class 3 malocclusion
Posterior crossbite
Cosmetic:
Lip defects
Nasal deformity - deviated nose in unilateral cleft lip, flat and broad nose in bilateral cleft lip and palate.
Middle face deformity
Management of cleft lip and palate
Primary correction
Feeding plate/ presurgical alveolar moulding
Primary lip and nose repair
Primary palate repair
Secondary correction
Secondary alveolar grafting
Pharyngoplasty
Orthodontic treatment
Orthognathic surgeries
Plastic surgery like rhinoplasty etc.
The team approach is needed to handle the complexity of cleft lip and palate. The team is composed of the following:
Plastic surgeon
Paediatrician
Pedodontist
Otologist
Orthodontist
Speech pathologist
Audiologist
Psychiatrist
Prosthodontist
Primary correction
Feeding plate:
An acrylic palatal plate which acts as an obturator is used. It can also be used as an orthopaedic appliance to mould the alveolar fragments.
Presurgical nasoalveolar moulding:
It includes a reduction of the size of the intra-alveolar cleft due to moulding of bony segments, active moulding and positioning of surrounding tissues affected by the cleft.
It is effective only in infants to whom cartilage is malleable.
1. Impression of infant's mouth
2. Custom-made plastic plate fabrication
3. Infants have to wear the plate for 24 hours for 6 months.
4. The plate is held in the mouth by a surgical skin tape that also helps in guiding the growth of the face.
5. The plate should be reshaped each week, reducing the cleft.
Primary lip repair:
It should not be done in the first 6 weeks of life.
Millard advocates the rule of 10
10 weeks of age
10 g/dl of haemoglobin
10 pounds of weight
Lip repair procedures include:
1. Lip adhesion procedure
2. Rose Thompson procedure
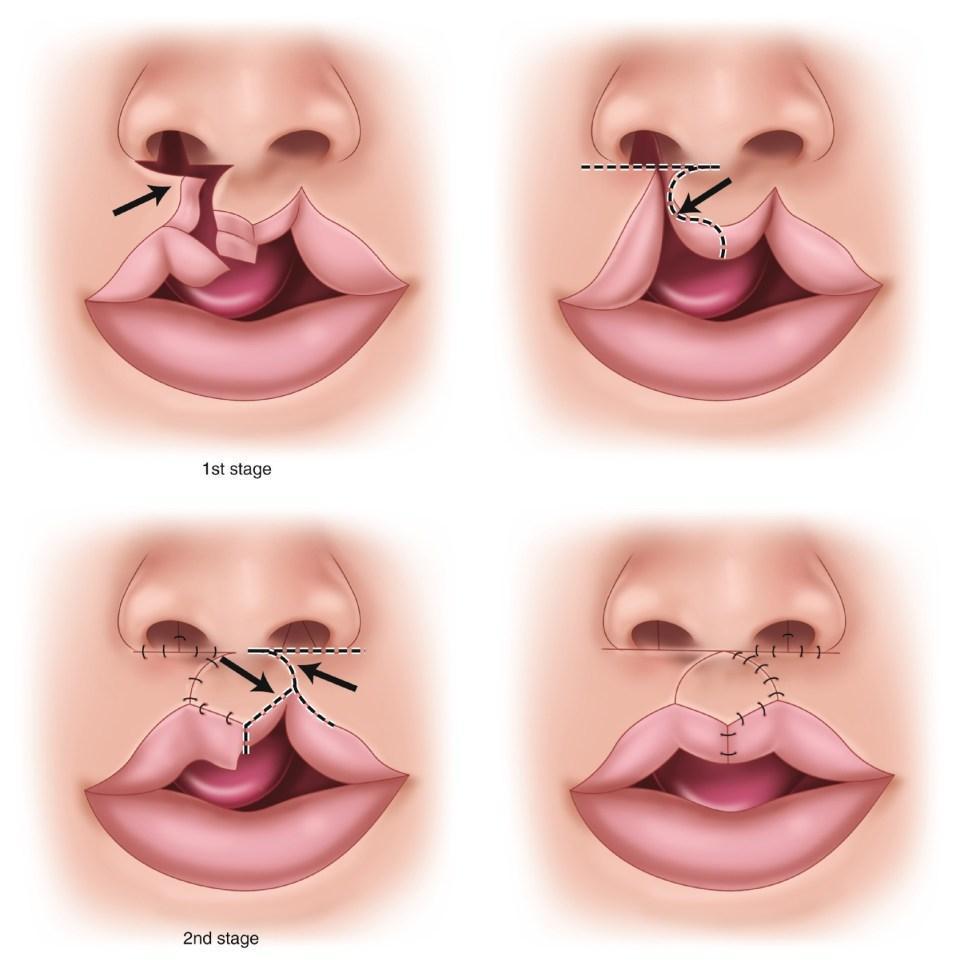
3. Tennison Randall triangular flap - triangular design avoids wound contracture and lip length shortening seen with the rotation and advancement flap operation.
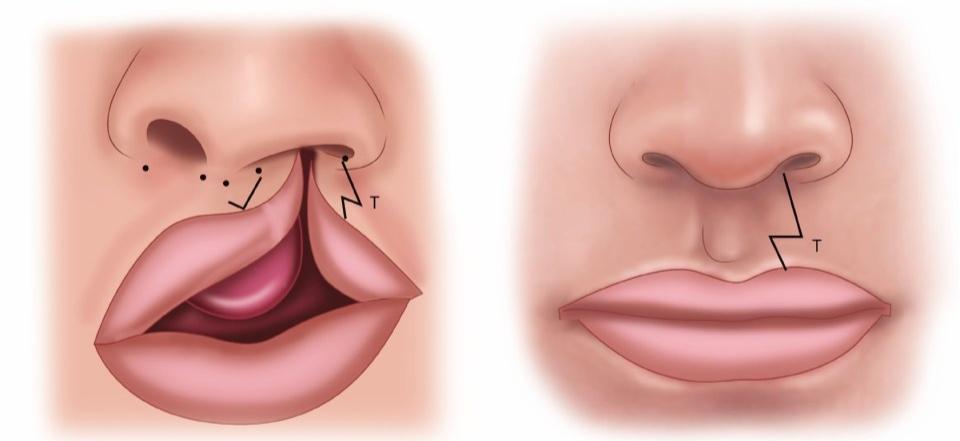
4. Millard rotation advancement flap - The tissue is rotated to create a longer vertical width and the cleft side is advanced horizontally.
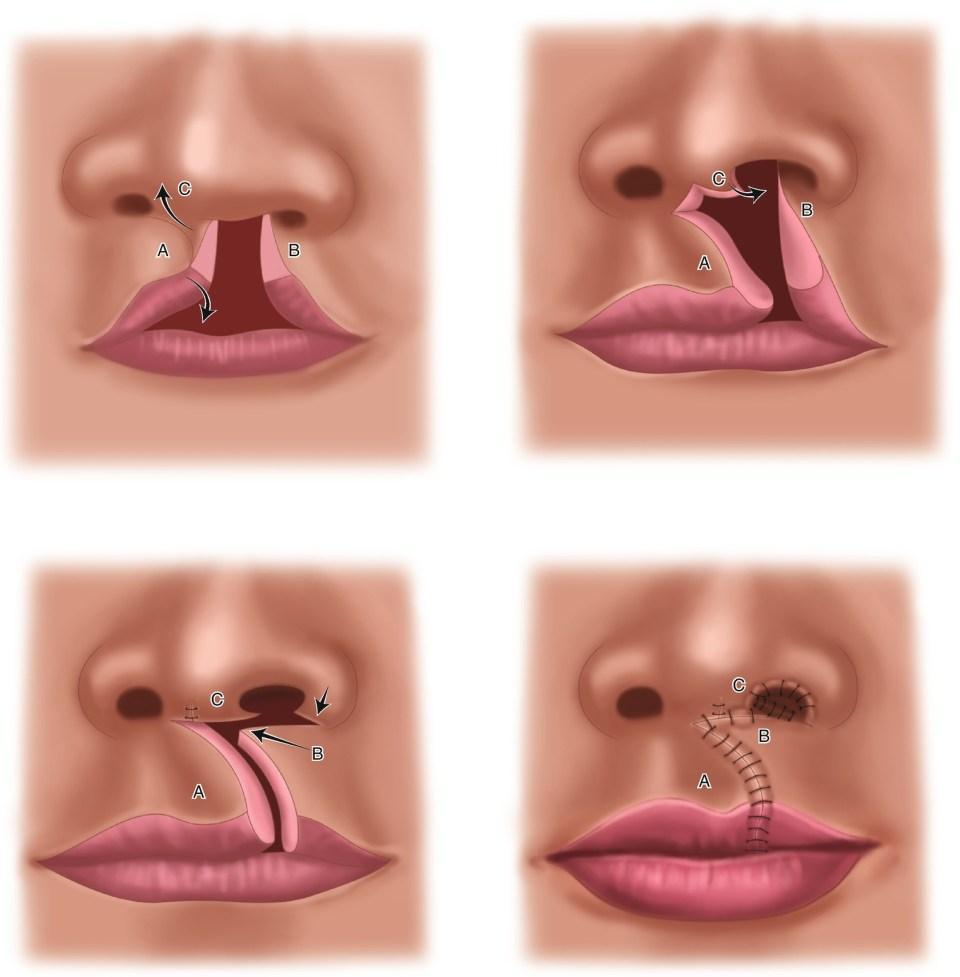
5. Delaire technique of muscular reconstruction - The nasal tissue is gently dissected to create a laxity. With the incisions open after the initial dissection of the Millard technique, a pair of tenotomy scissors are used to dissect over the lower lateral cartilages to free this tissue from its abnormal insertions. After the nasal tissue is dissected, the muscle and skin are reapproximated with additional sutures placed in the area of the nasal floor to create symmetry between the nostrils.
6. Noordhoff technique
Primary palate repair:
The main purpose is to prevent the regurgitation of food through the nose, providing normal anatomy for normal speech,
The procedures include
1. Modified Von Langerback operation
The two full-thickness flaps are created and mobilized with layered dissection of the soft palatal tissues. The anterior and posterior portions remain connected to the periosteum to increase circulation. There is usually an area laterally that is allowed to granulate in. This healing through secondary intention can increase pain and create scar formation that restricts growth.
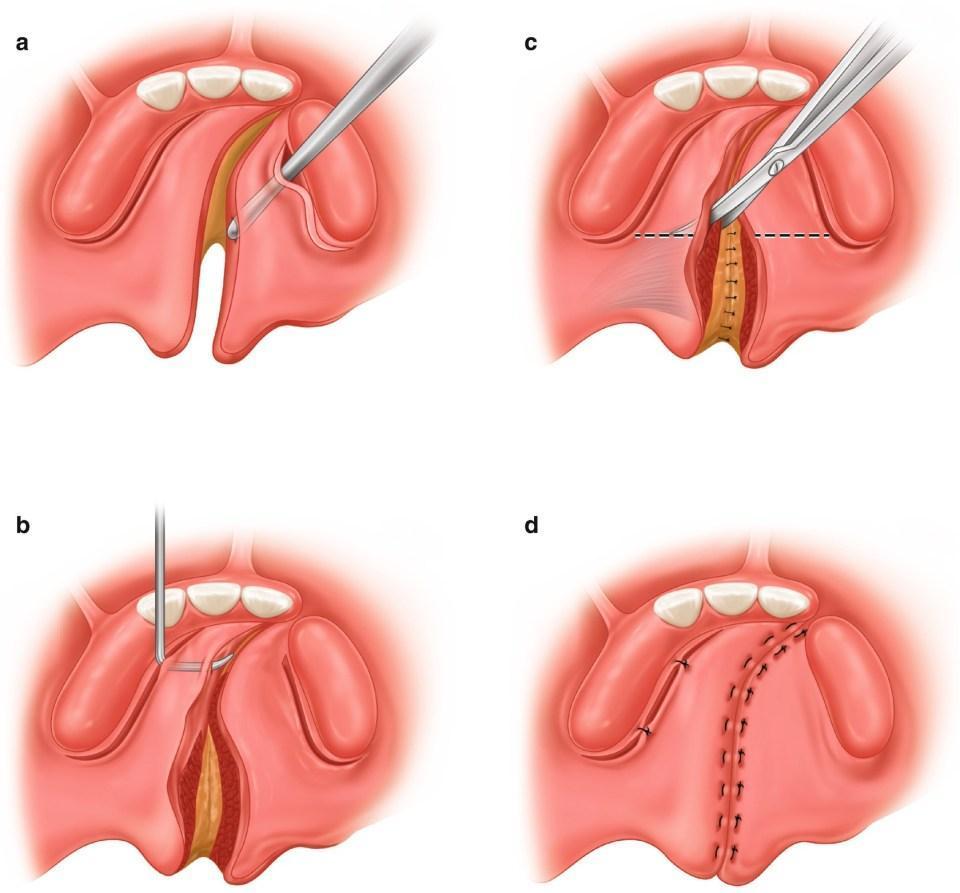
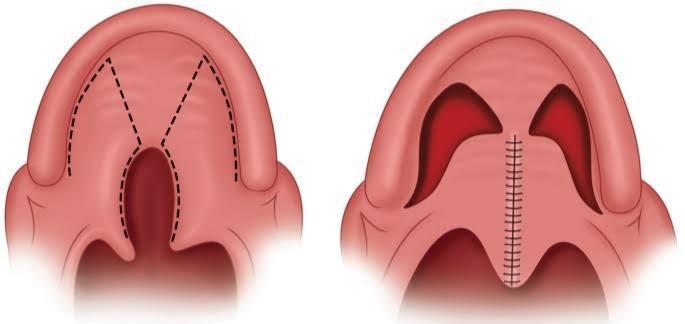
2. V-Y pushback palatoplasty
Releasing muscles of the soft palate from the posterior edge of the hard palate and from the periosteum on the nasal side allows the creation of a more physiologic muscle sling and soft palate. There is an anterior two-layer closure and a posterior three-layer closure.
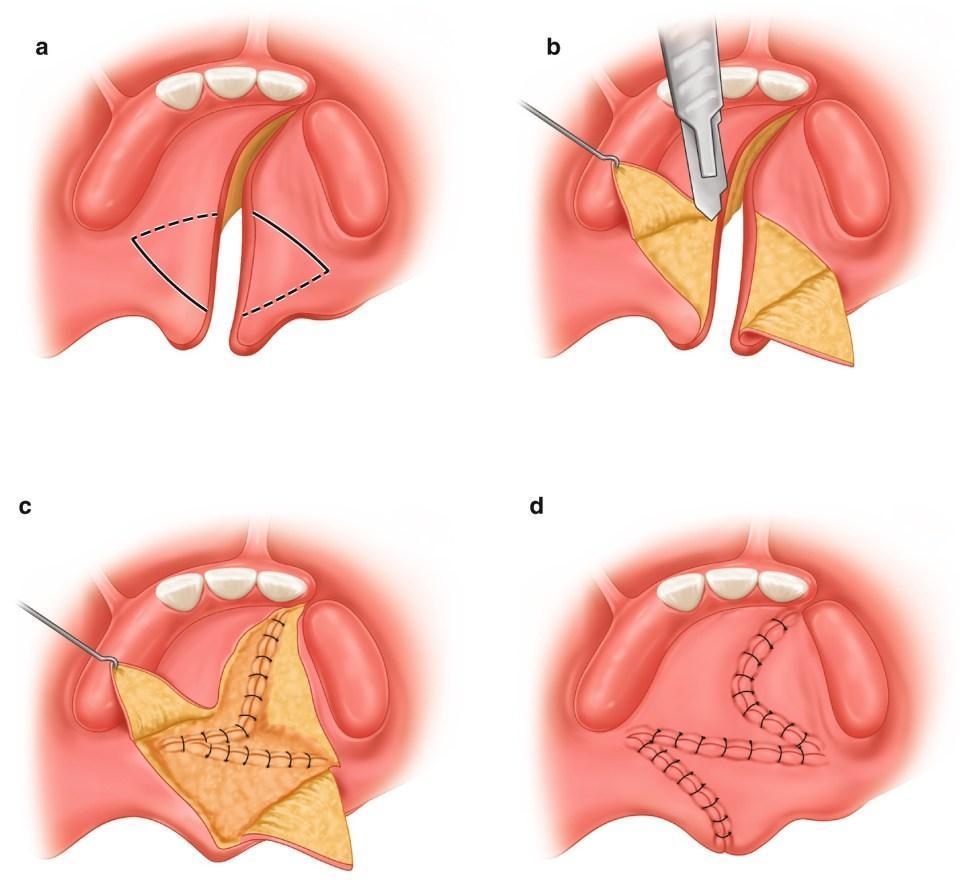
3. Furlow double opposing Z Plasty
4. Anterior vomer flap
5. Intravelar veloplasty
Secondary correction
Alveolar bone grafting:
It aims to eliminate the oronasal fistula, create bone support for tooth eruption, restructure hypoplasia, and nasal base elevation.
Depending on the time of surgery, it can be
Primary bone grafting: younger than 2 years
Early secondary bone grafting: between 2 and 5 years of age
Secondary bone grafting: greater than 5 years of age
Aim of primary bone grafting:
To achieve early stabilization of maxillary arches and to obliterate alveolar oronasal fistula.
Aim of secondary bone grafting:
Creating bone support for tooth eruption, placement of implant
Provision of support for soft tissue nasal base and reconstruction of hypoplastic piriform aperture
Creating suitable architecture for premaxilla
Grafts used:
1. Ribs for primary grafting
2. Particulate marrow and cancellous iliac crest bone graft for secondary grafting
3. Cranial bone
4. Hydroxyapatite to restore alveolar ridge form
Orthodontic management:
Late primary and early mixed dentition:
Permanent incisors may be rotated on in crossbite - treated with a removable appliance
Early permanent dentition:
Tendency to develop posterior crossbite - fixed orthodontic treatment
After growth completion:
Comprehensive orthodontic treatment:
By pre-adjusted edgewise appliance for precise positioning
Reverse pull headgear and chin cup can be used.
Orthognathic surgeries:
Le Fort 1 osteotomy - to advance the maxillary and correct crossbite
Maxillary distraction osteogenesis - after 3 days of le Fort 1 osteotomy, a rigid external distraction device or intraoral device is placed and activated 1 mm a day. It is stopped when crossbite is overcorrected and the patient is placed in retention for 3 months.
Reference:
Oral and maxillofacial surgery by Dr SM Balaji
Essential Orthodontics by Dr Sridhar Premkumar
1 comment