Introduction
For children, aged 0-6 years, oral injuries account for 18% of all physical injuries and the mouth is the second most common area of the body to be injured. Traumatic dental injuries have a world prevalence of 22.7% affecting the primary teeth. Unintentional falls, collisions, and leisure activities are the most common reasons for TDIs, especially as children learn to crawl, walk, run, and embrace their physical environment. They most commonly occur between 2 and 6 years of age.
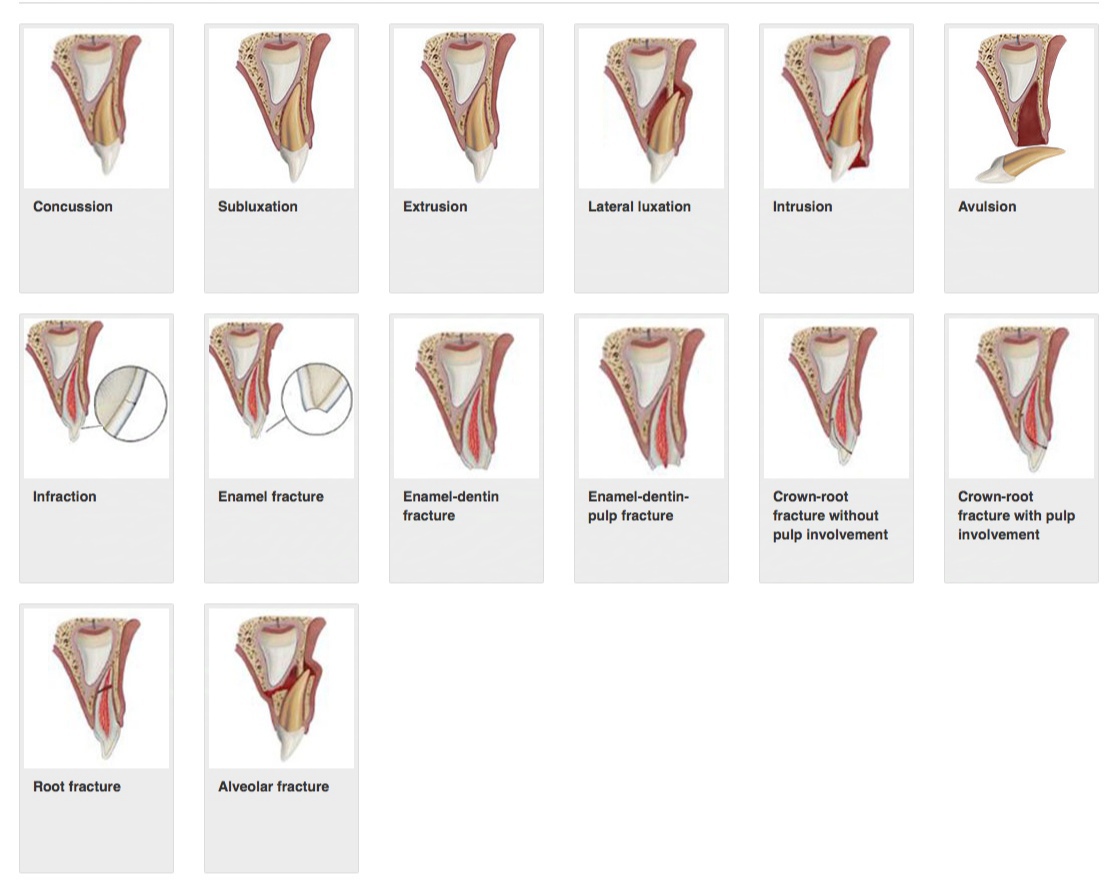
Classification of traumatic dental injuries in primary dentition
Treatment options
The management of traumatic dental injuries to the primary dentition aims to prevent damage to the developing permanent tooth germ, alleviate pain, and minimize possible complications, such as infection.
Fractures | Features | Treatment |
Concussion | Tooth is tender to touch but no displacement | Observation |
Subluxation | Tender Increased mobility Not displaced | Observation |
Extrusive luxation | Appears elongated Excessively mobile Occlusal interference | If not interfering with occlusion, let the tooth for spontaneous repositioning If excessively mobile oe extruded >3mm, extract under LA |
Lateral luxation | Displaced usually in labial or lingual direction Immobile Occlusal interference | If no occlusal interference, spontaneous repositioning of tooth by itself (it takes about 6 months) If severely display, extract under LA to avoid aspiration or ingestion of tooth Under LA, reposition the tooth and splint for 4 weeks with flexible splint. |
Intrusive luxation | Displaced through the labial cortical plate or impinged permanent tooth bud. Tooth almost or completely disappeared into socket and can be palpated labially | Allow spontaneous repositioning by itself. |
Avulsion | Completely out of socket | Should not be replanted. |
Enamel fracture | Fracture of enamel only | Smoothen any rough edges |
Enamel dentin fracture | Pulp not exposed, enamel and dentin fracture Sensitivity | Cover all exposed dentin by GIC. Lost tooth structure can be restored with composite. |
Complicated crown fracture | Fracture involving enamel, dentin and pulp | Preserve pulp by partial pulpotomy |
Crown root fracture | Fracture involving enamel, dentin and root structure with or without pulp exposure. Loose but still attached fragment can be present | Remove the loose fragment If restorable and there is no pulp involvement, cover the exposed dentin with GIC. If restorable and pulp is exposed, perform pulpotomy or pulpectomy If unrestorable, extract the entire tooth without disturbing the permanent tooth bud |
Root fracture | Rare in primary dentition Depending on the location of fracture, the coronal segment may be mobile or displaced and have occlusal interference | If no displacement, no treatment If displaced but not mobile, allow for spontaneous repositioning by itself If displaced, mobile with occlusal interference, extract the loose fragment or reposition it with flexible splint for 4 weeks. |
Alveolar fracture | Fracture of alveolar bone involving labial and palatal/ lingual plate Mobility Dislocation Occlusal interference | Repositioning under LA and stabilizing with a flexible splint for 4 weeks. |

Post a Comment