
Myocardial Infarction
Introduction
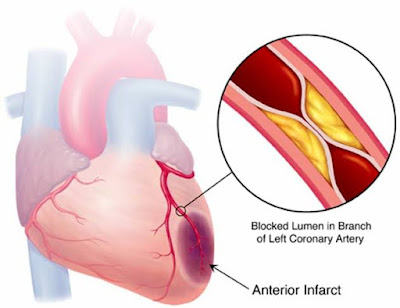
Myocardial infarction, in layman's terms, Heart Attack, is defined as the myocardial cell death due to prolonged myocardial ischemia. It is caused by partial or complete cessation of blood flow to a part of the myocardium.
The coronary arteries are those that supply blood to the heart/ myocardium. Any occlusion to the coronary artery can cause decreased/ absence of blood flow to that particular part of the myocardium causing oxygen deprivation leading to myocardial ischemia and necrosis.
Blood supply to the heart
The heart gets its blood circulation during ventricular diastole.
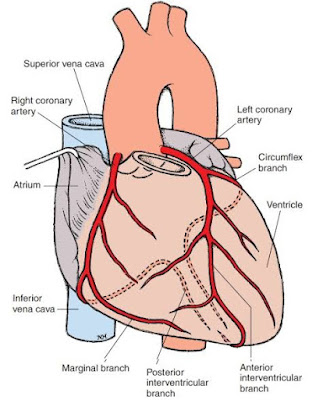
The Coronary arteries originating from the base of the aorta, supply the heart. It is divided into left and right coronary arteries.
The left coronary artery further divides into the circumflex artery and the anterior interventricular artery (left anterior descending artery).
The right coronary artery further divides into conus arteries(2), posterior interventricular artery (posterior descending artery) and right posterolateral artery.
Etiology
The modifiable risk factors include smoking, abnormal apolipoprotein ratio, hypertension, diabetes mellitus, obesity, lack of physical activity, and alcohol consumption.
The non-modifiable risk factors include advanced age, male sex, and genetics.
Symptoms
Intense, crushing type of substernal chest pain/ discomfort radiating to the jaws, left shoulder and arm. (Diabetic patients may not experience the chest pain due to the neuropathy)
Difficulty in breathing
Fear of impending death
Profuse sweating
Nausea
Warmness
Epigastric pain
Pathophysiology
An acute occlusion of one of the coronary arteries for a period of 20 to 40 minutes leads to acute myocardial infarction. The occlusion may be due to a thrombosis or the rupture of the atherosclerotic plaque. This causes myocardial ischemia leading to sarcolemmal disruption and myocardial relaxation. With a series of ultra-structural changes, coagulative necrosis of the myocardium takes place. The necrosis spreads to the sub-endocardium and sub-epicardium. The course of action is prolonged due to the increased collateral supply of epicardium.
Depending on the site of infarction, the cardiac function is compromised.
If timely reperfusion is implemented, the myocardium heals by scarring. The compensation including cardiac remodeling, hypertrophy etc. takes place.
Investigations and Evaluation
12 lead ECG showing the following characteristics:
ST segment elevation in 2 continuous leads
ST segment depression along with T wave changes like hyperacute T wave amplitude, prominent symmetrical T waves
Other myocardial ischemic findings like arrhythmias, AV conduction delay etc
Biomarkers include the following:
Raising or falling pattern of cardiac troponin (cTn) levels
Elevated creatine kinase MB isoform
Elevated levels of LDH after 24 hours
Clinical evidence of myocardial injury
Hypoxemia
Hypotension or shock
Anemia
Ventricular tachycardia
Heart failure
Kidney disease
Clinical classification of myocardial infarction
Type 1 myocardial Infarction:
MI due to rupture or erosion of atherosclerotic plaque.
It can further be classified based on the ECG findings as ST elevation myocardial infarction (STEMI) and Non ST elevation myocardial infarction (NSTEMI)
Criteria for diagnosis include
Symptoms of acute MI
ECG changes indicating ischemia
Imaging evidence of coronary thrombus by angiography
Type 2 myocardial infarction:
MI due to an imbalance in the myocardial oxygen demand and supply because of secondary disease.
Causes include GI bleed or tachyarrhythmia in presumed CAD patients, coronary vasospasm, coronary embolism, respiratory failure, severe anemia, Hypotension or shock etc.
Type 3 myocardial infarction:
Cardiac biomarkers in blood are fundamental for diagnosing type 3 MI.
Type 4a myocardial infarction:
MI is associated with percutaneous coronary intervention.
Type 4b myocardial infarction:
MI is associated with documented stent thrombosis.
Type 5 myocardial infarction:
MI is associated with coronary artery bypass grafting.
Classification according to the location of the infarct
Right ventricular myocardial infarction:
MI due to occlusion in the right coronary artery. The signs include increased RV pressure, tricuspid regurgitation and decreased cardiac output.
Inferoposterior myocardial infarction:
MI due to occlusion of the left circumflex artery leading to right ventricular dysfunction.
Anterior wall myocardial infarction:
MI due to the occlusion of the left coronary artery especially the anterior descending artery.
It has the worst prognosis.
Classification based on the extent of infarction
Transmural infarction:
MI involves the whole thickness of the myocardium.
Evidence of abnormal Q waves on ECG.
Laminar infarction:
Subendocardial infarct involving only the endocardium.
Evidence of ST - T abnormalities only.
Management
Acute management:
Reperfusion therapy:
It is indicated in all acute MI patients with less than 12 hours of symptoms.
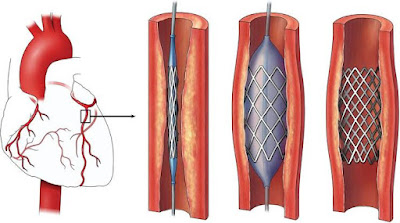
Percutaneous coronary intervention (PCI)
It is passing a fine guidewire across a coronary stenosis under radiographic control and using it to position a balloon, which is then inflated to dilate the stenosis. It can be combined with a coronary stent.
Fibrinolysis like tenecteplase, alteplase, or reteplase.
Anticoagulants like unfractionated heparin, enoxaparin, and bivalirudin
Symptomatic relief:
Opioids for pain relief
Nitrates - Intravenous nitrates are more effective than sublingual nitrates
Beta-blockers - reduce myocardial oxygen consumption by decreasing heart rate, BP, and myocardial contractility.
Platelet inhibition - Aspirin, thromboxane A2 inhibitor, with a loading dose of 150 to 300mg and maintenance dose of 75 to 100 mg per day for the long term. Ticagrelor, an orally active P2Y12 inhibitor, can be used. Other P2Y12 inhibitors like clopidogrel, prasugrel can also be used.
Long-term management:
Lipid-lowering agents like Statins reduce LDL to stabilize the atherosclerotic plaque
Antithrombotic drugs like Aspirin, clopidogrel etc.
ACE inhibitors for patients with heart failure, hypertension etc
Antihypertensive drugs like beta blockers
Lifestyle modification:
Cessation of smoking, alcoholism
Diet and weight control
Complications
Reinfarction
Arrhythmias - supraventricular or Ventricular
AV block
Cardiac failure
Cardiac shock
Pericarditis
Embolism
Death due to Cardiac arrest
Reference:
Davidson's Principles and Practice of Medicine
PubMed Articles
AHA website
Google scholar
6 comments