
Anemia - Iron Deficiency Anemia
Introduction
Anemia is functionally defined as an insufficient RBC mass to adequately deliver oxygen to the peripheral tissues.
It may be characterized by decreased RBC mass, decreased hemoglobin concentration, or decreased hematocrit for the appropriate age, sex and altitude of residence.
It may be due to increased RBC clearance, decreased RBC production, or both (intrinsic or extrinsic pathways).
According to WHO, hemoglobin <13 g/dl in males, <12 g/dl in non-pregnant females, and <11 g/dl in pregnant females is considered as evidence of anemia.
.webp)
Etiology
Decreased hemoglobin synthesis:
Lack of nutrients: iron, vitamin B12, folic acid
Bone marrow failure: due to drugs, chemotherapy, infections etc.
Increased hemoglobin loss:
Hemorrhage - RBC loss
Hemolysis - RBC destruction
Decreased RBC production:
Disturbance in stem cell proliferation, or differentiation due to bone marrow infiltration by cancer cells, infection, etc.
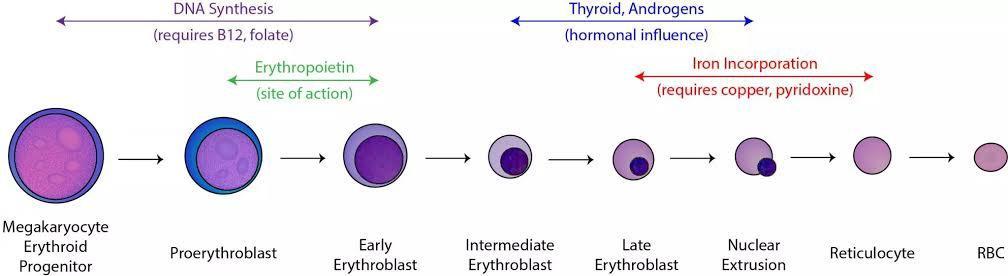
Life cycle of RBC
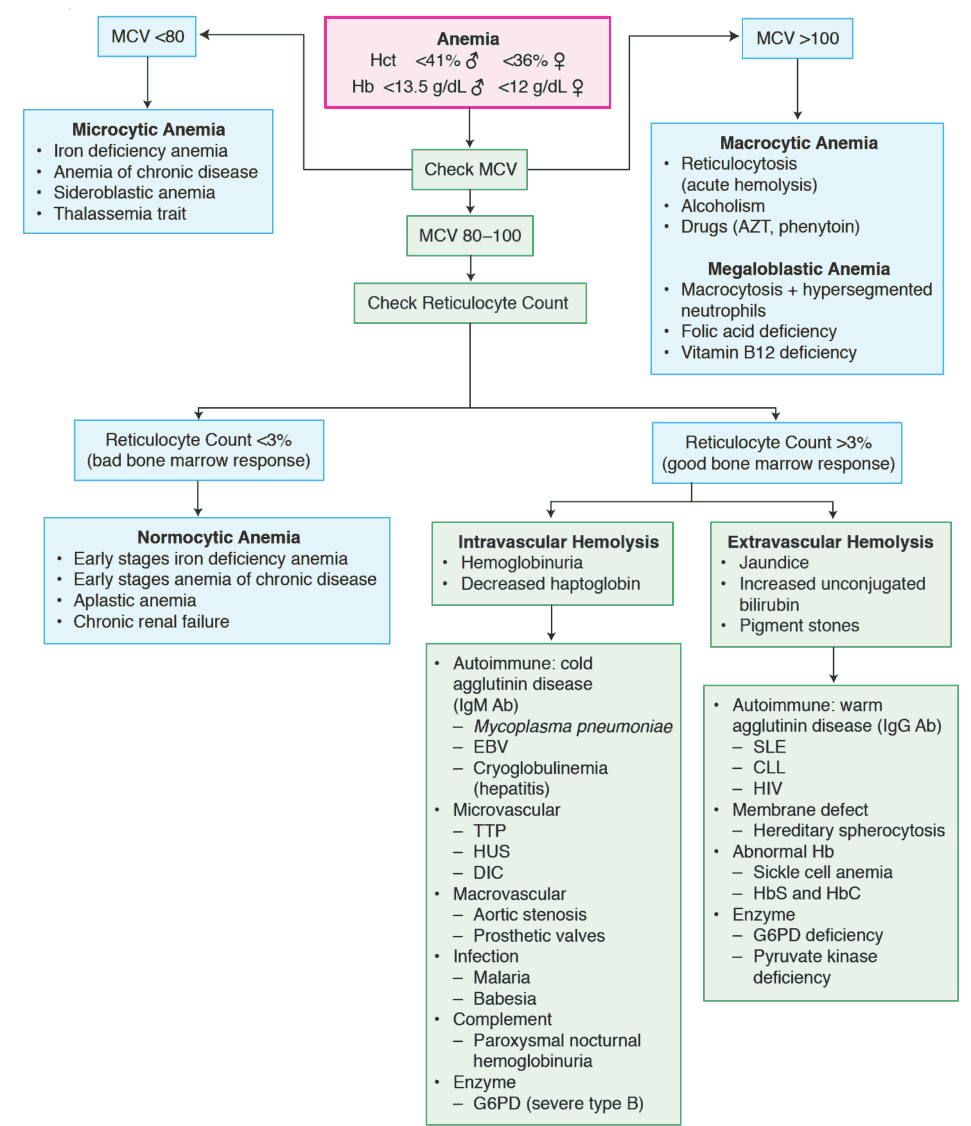
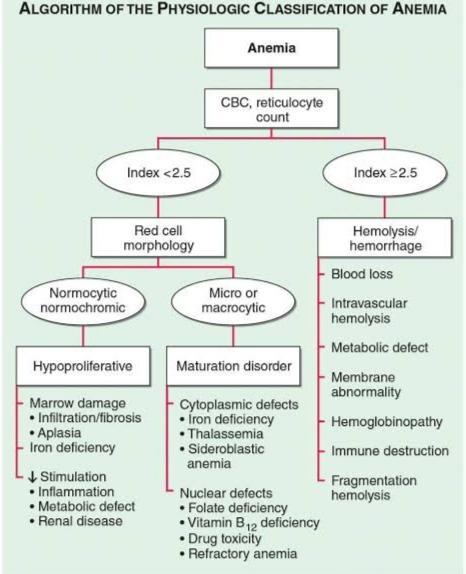
Classification of anemia
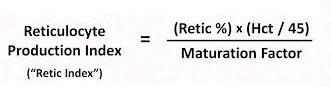
Reticulocyte Production Index
It gives the functioning of the bone marrow.
Symptoms of Anemia
Fatigue or low-energy
Increased heart rate
Shortness of breath
Headache/dizziness
Iron Deficiency Anemia
Normal iron content in the body is 50 mg/kg in males and 40 mg/kg in females.
Distribution of iron:
67% in hemoglobin
27% in ferritin
3.5% in myoglobin
0.08% in transferring
Forms of iron in the body:
The iron is absorbed in Ferrous form (Fe2+)
The circulatory and storage form of iron is Ferric (Fe3+)
It is primarily stored as ferritin in bone marrow, macrophages, duodenum, liver and brain.
Stages of iron deficiency anemia
Prelatent:
Reduction in iron stores without reduction in serum iron levels.
Features - normal hemoglobin, normal MCV, normal transferrin saturation, increased iron absorption, decreased serum ferritin, decreased marrow iron.
Latent:
Iron stores are exhausted but the serum iron level is normal.
Features - normal hemoglobin, normal MCV, increased total iron binding capacity, decreased serum ferritin, decreased transferrin saturation, marrow iron absent.
Iron deficiency anemia:
Blood hemoglobin concentration is below the lower limit of normal.
Features - decreased hemoglobin, decreased MCV, increased total iron binding capacity, decreased serum ferritin, decreased transferrin saturation, marrow iron absent
Causes
Increased iron demand:
Infancy
Adolescence
Pregnancy
Erythropoietin therapy ( in CKD)
Increased iron loss:
Chronic blood loss
Menses
Acute blood loss like road traffic accidents, hemorrhoids etc
Phlebotomy as treatment of polycythemia vera
Blood donation
Decreased iron intake/ absorption:
Inadequate diet
Malabsorption from disease (coeliac sprues, Crohn's disease)
Malabsorption from surgery (gastrectomy, other bariatric surgery)
Acute or chronic inflammation
Clinical features
Geographic tongue - bald tongue due to loss of filiform papilla from the periphery to the centre
Flattening/ koilonychia of nails
Angular stomatitis
Dysphagia/ esophageal webs (Plummer-Vinson Syndrome)
Achlorhydria/ gastritis
Pica - craving for materials with no nutritional value (clay, ice, etc.)
Plummer Vinson Syndrome: A triad of iron deficiency anemia, post cricoid/ esophageal webs, dysphagia.
Lab findings in iron deficiency anemia
Decreased MCV
Decreased RDW
Microcytic hypochromic
Pencil cells, target cells
Anisocytosis
Decreased RBC count
Decreased serum iron
Increased total iron binding capacity
Decreased transferrin saturation
Decreased ferritin (most sensitive)
Marrow iron absent
Treatment
Oral iron supplements:
It is given for iron deficiency erythropoiesis, pre-latent stages with negative iron balance. It should be continued for 6 to 12 months post-correction.
Parenteral iron therapy:
It is preferred nowadays.
Post a Comment