
Megaloblastic Anemia
Introduction
These are disorders caused by impaired DNA synthesis in the erythroid lineage due to the deficiency of vitamin B12 or folic acid which gives rise to anemia and macro-ovalocytic RBC (MCV >100fL) and bone marrow shows intense erythroid hyperplasia and megaloblastic changes.
Here, DNA maturation lags behind.
Absorption of Vitamin B12
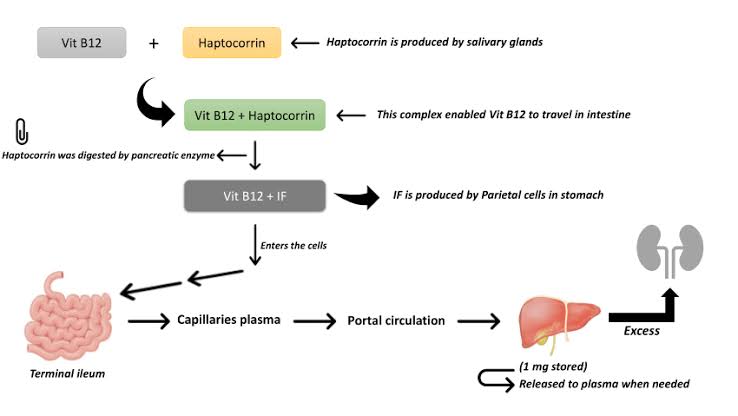
Common causes of vitamin B12 deficiency in India
Nutritional deficiencies
Malabsorption
Defective absorption from food (gastric achlorhydria, partial gastrectomy, drugs blocking gastric secretion)
Inadequate intrinsic factor production
Disorders of terminal ileum (tropical/coeliac sprues, intestinal resection, granulomatous diseases)
Competition for cobalamin by bacteria (blind loop syndrome)
Drugs like colchicine and neomycin
Uncommon causes of vitamin B12 deficiency in India
Pernicious anemia
Absence or abnormalities in intrinsic factor
Crohn's disease
Selective B12 malabsorption (Imerslund - Grasbeck syndrome)
Fish tapeworm ingestion
Transcobalamin deficiency
Common causes of folic acid deficiency in India
Nutritional deficiencies
Increased requirement (infants, children, pregnancy, hemodialysis, malignancy, chronic hemolytic anemia, chronic exfoliative dermatitis)
Malabsorption
Impaired metabolism (inhibitors of dihydrofolate reductase)
Methotrexate, pyrimethamine
Alcohol
Uncommon causes of folic acid deficiency in India
Rare enzyme defect (dihydrofolate reductase)
Drugs that impair DNA synthesis
• purine antagonists: 6 mercaptopurine, azathioprine
• pyrimidine antagonists: 5 fluorouracil, cytosine arabinoside
• others: hydroxyurea, procarbazine, zidovudine, acyclovir
Metabolic disorders (Lesch Nyhan Syndrome, hereditary orotic aciduria)
Megaloblastic anemia of unknown etiology
Refractory megaloblastic anemia in myelodysplastic syndrome
Diagnosis
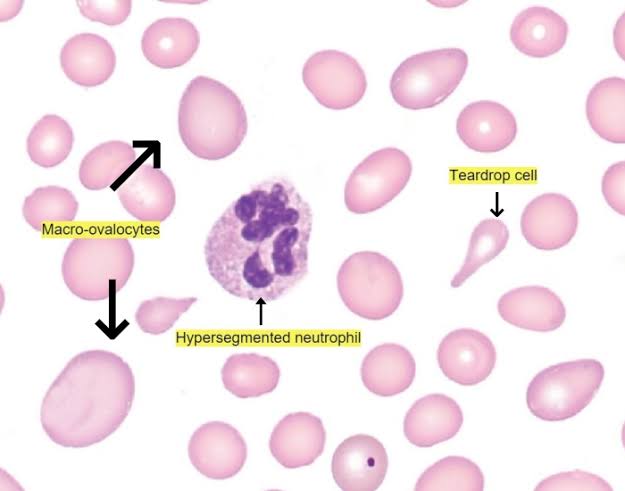
Blood picture:
Decreased hemoglobin
Increased MCV
Normal MCHC
Increased MCH
Macrocytic RBC: macro-ovalocytes, and Howell - Jolly bodies are seen
Decreased RBC with an increase in hypersegmented neutrophils
Normal or reduced platelet count
Bone marrow:
Hypercellularity
Hyperactive erythropoiesis and megaloblastic changes are seen in all stages of development
Megaloblasts are larger than erythroblasts with increased cytoplasm and nuclear size
Chromatin is more open being arranged in a fine reticular fashion giving a stopped appearance
Predominant cells are pro-megaloblasts and basophilic megaloblasts indicating maturation arrest
Active granulopoiesis showing giant metamyelocytes
Normal megakaryocytes
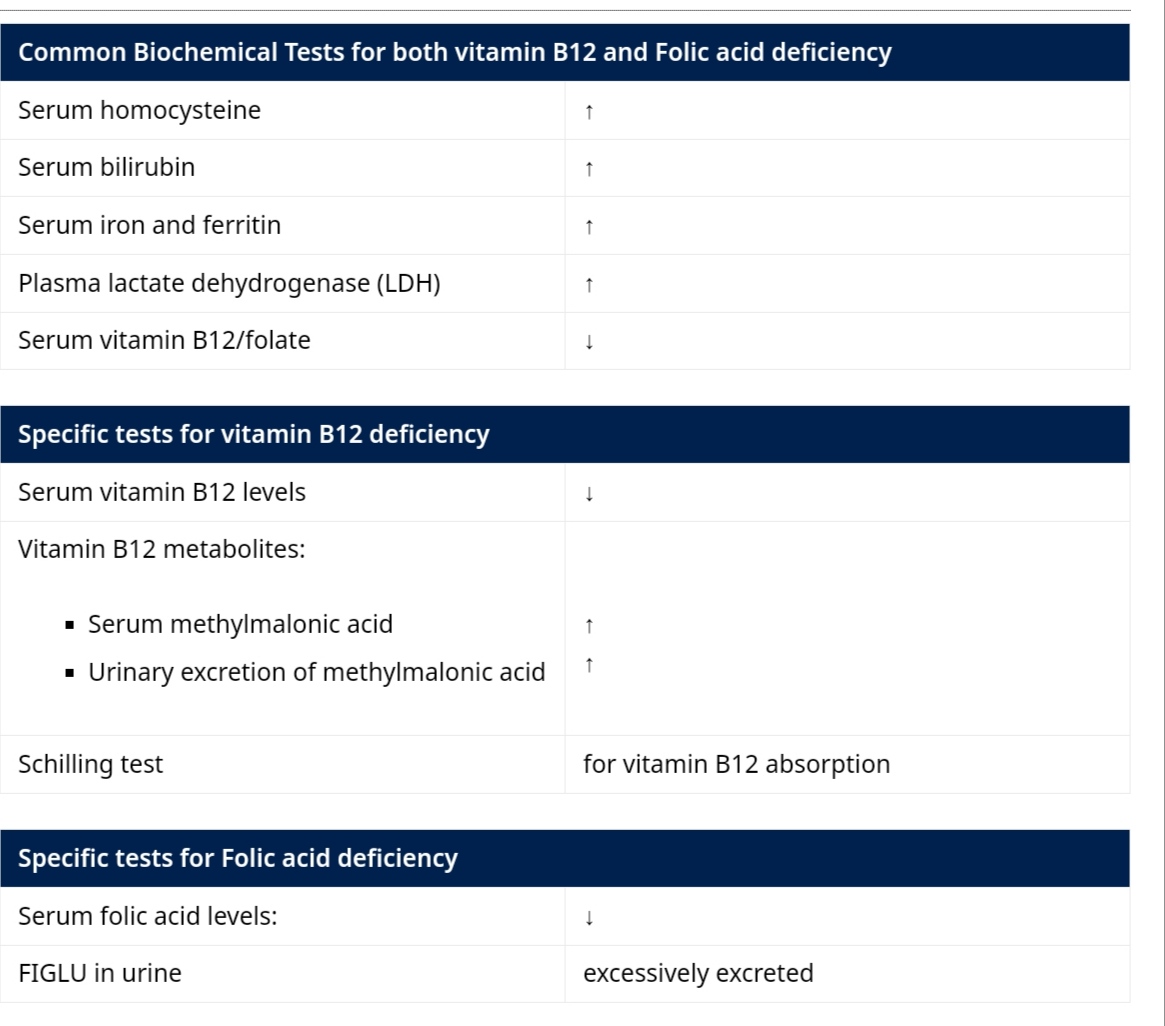
Biochemistry:
Serum vitamin B12
Red Cell folate assay
Microbial assay of vitamin B12 using Lactobacillus leichmannii
Treatment
Goal:
Reversal of hematologic manifestation
Replacement of body stores
Prevention/ resolution of neurologic manifestations
Dietary intake:
Animal rich food
Green leafy vegetables
Milk and milk-based products
Medications:
Oral administration of vitamin B12 (1-10 micrograms/ day)
Parenteral administration (100-1000 micrograms deep i.m)
Pernicious Anemia
Vitamin B12 deficiency anemia due to lack of intrinsic factor due to atrophic gastritis or antibodies against intrinsic factor
Blood and bone marrow pictures are similar to megaloblastic anemia.
Clinical features:
Paresthesia of hand and feet
Spinal cord - Posterior or lateral column defect
Dementia
Neuropsychiatric features
Optic nerve involvement
Atrophic glossitis - red beefy tongue
Angular cheilitis
Intestinal-type gastric adenocarcinoma
Gastric carcinoid type 1
Diagnosis:
Schilling’s test
Antiparietal cell antibody type 3 - most sensitive
Anti-intrinsic factor antibody type 1 / 2 - most specific
Treatment - cyanocobalamin/ hydroxycobalamin
1000 micrograms i.v. daily for a week
Followed by once a week for a month
Followed by once a month for 6-8 months
If symptoms are not improved - Lifelong cyanocobalamin/ hydroxycobalamin treatment.
Post a Comment