
Traumatic Dental Injuries
Introduction
Traumatic dental injury (TDI) is any injury to the teeth and the surrounding periodontium and soft tissues. It is usually sudden, impactful, circumstantial and accidental. It is common in children and young adults.
Classification of traumatic dental injuries is proposed by various authors.
Ellis and Davey classification (1960):
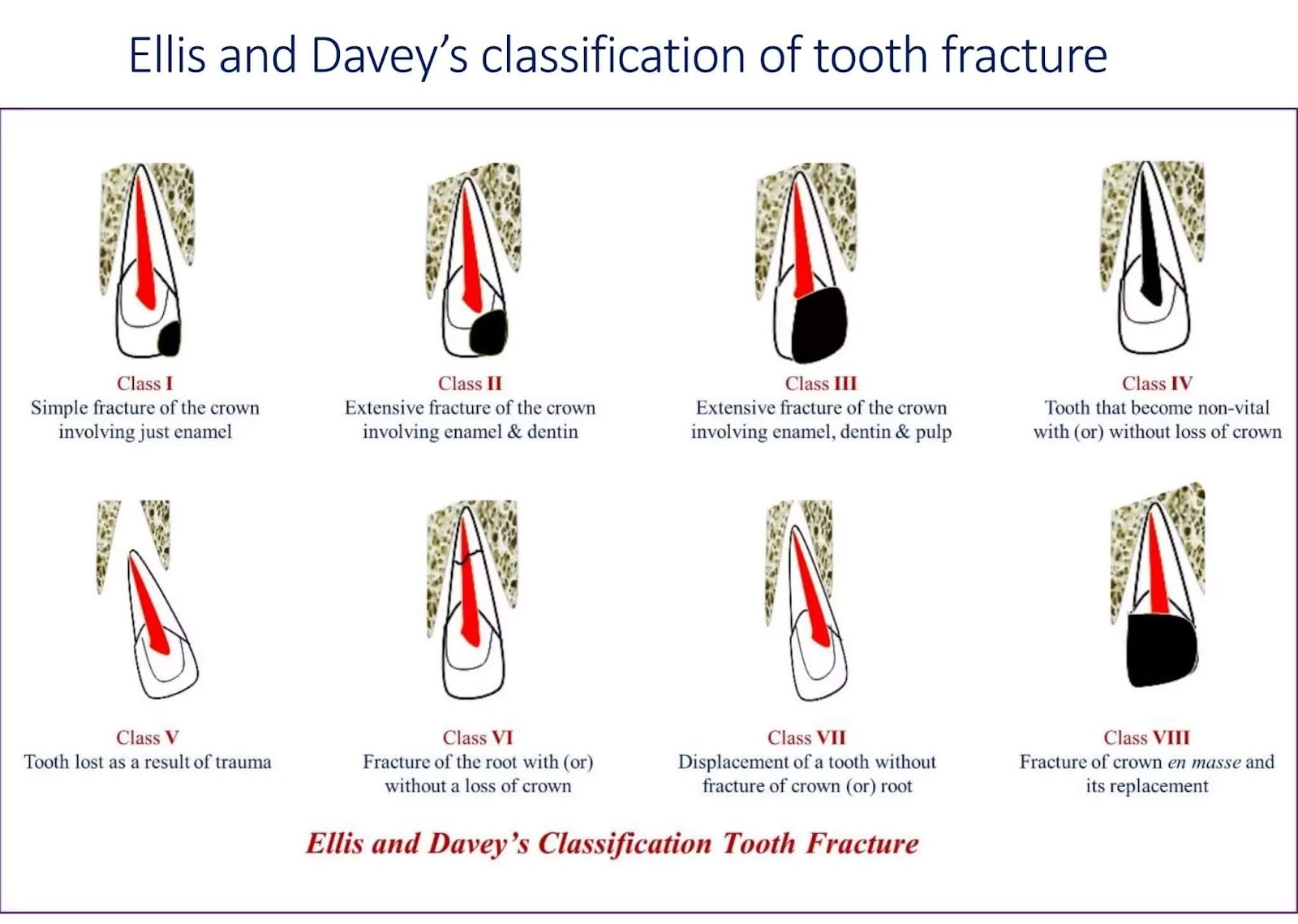
Class I – simple crown fracture without involving dentin
Class II – extensive crown fracture involving enamel and dentin without involving pulp
Class III – extensive crown fracture with pulp exposure
Class IV – non vital tooth (with or without any fracture)
Class V – avulsed tooth
Class VI – root fracture with or without crown fracture
Class VII – displacement of tooth without fracture
Class VIII – crown en masse
Class IX – primary tooth fracture
Andreason’s classification (1981)
Injuries to the hard dental tissues and pulp
Enamel infraction: incomplete fracture or cracks in enamel
Enamel fracture: uncomplicated crown fracture
Enamel – dentin fracture: uncomplicated crown fracture
Complicated crown fracture: involving enamel and dentin with pulp exposure
Uncomplicated crown – root fracture: involving enamel, dentin and cementum without pulp exposure
Complicated crown – root fracture: involving enamel, dentin and cementum with pulp exposure
Root fracture: involving dentin, cementum and pulp
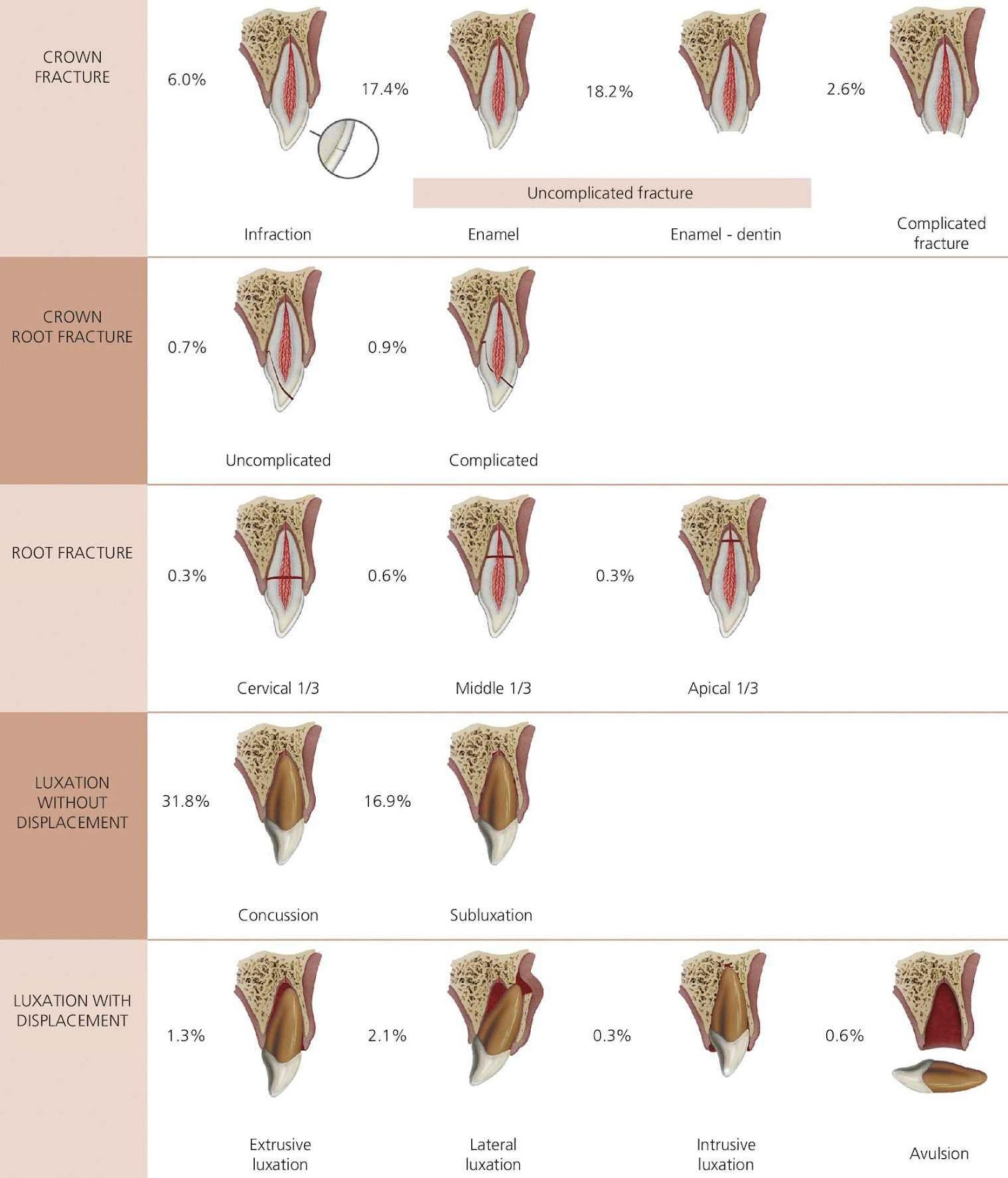
Image source: Skaare & Jacobsen 2003
Injuries to periodontal tissues
Concussion: injury to supporting structures without abnormal loosening or displacement of tooth
Subluxation: injury to supporting structures abnormal loosening without displacement of tooth
Extrusive luxation: partial displacement of tooth out of socket
Lateral luxation: displacement of tooth in any direction other than axial
Intrusive luxation (central dislocation): displacement into the socket
Avulsion (exarticulation): complete displacement out of socket
Image source: Skaare & Jacobsen 2003
Injuries to supporting bone
Comminution of mandibular or maxillary alveolar socket: crushing or compression of socket
Fracture of mandibular or maxillary socket wall: fracture of facial or lingual wall
Fracture of mandibular or maxillary alveolar process: involving base of mandible or maxilla
Injuries to gingiva or oral mucosa
Laceration: shallow or deep wound leading to tear of mucosa; by a sharp object
Contusion: bruise due to impact of blunt object
Abrasion: due to rubbing of mucosa – a superficial wound
Treatment options
Initial clinical examination
Radiographic examination
Pulp status evaluation
Stabilisation
Treatment
Follow up
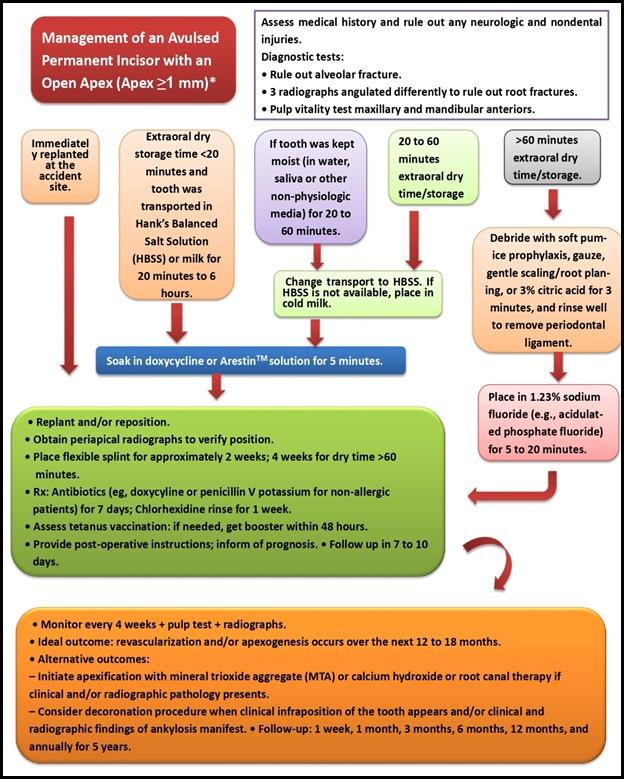
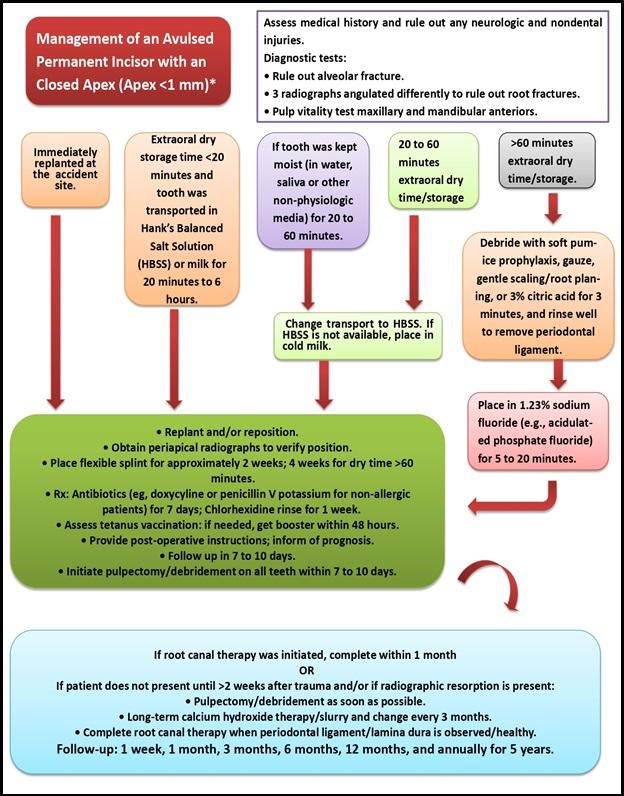
Avulsion
Post a Comment