
Corticosteroids - Double Edged Sword!
Introduction
Corticosteroids are hormones produced by the Adrenal gland situated on top of the kidneys. Adrenal cortex consists of three layers: zona glomerulosa, zona fasciculata and zona reticularis from outside to within. Corticosteroids can be broadly divided into glucocorticoids and mineralocorticoids. Mineralocorticoids are secreted from zona glomerulosa. Zona fasciculata secretes glucocorticoids. Chemically, corticosteroids are synthesized from cholesterol. Glucocorticoid secretion is maximum in the early morning.
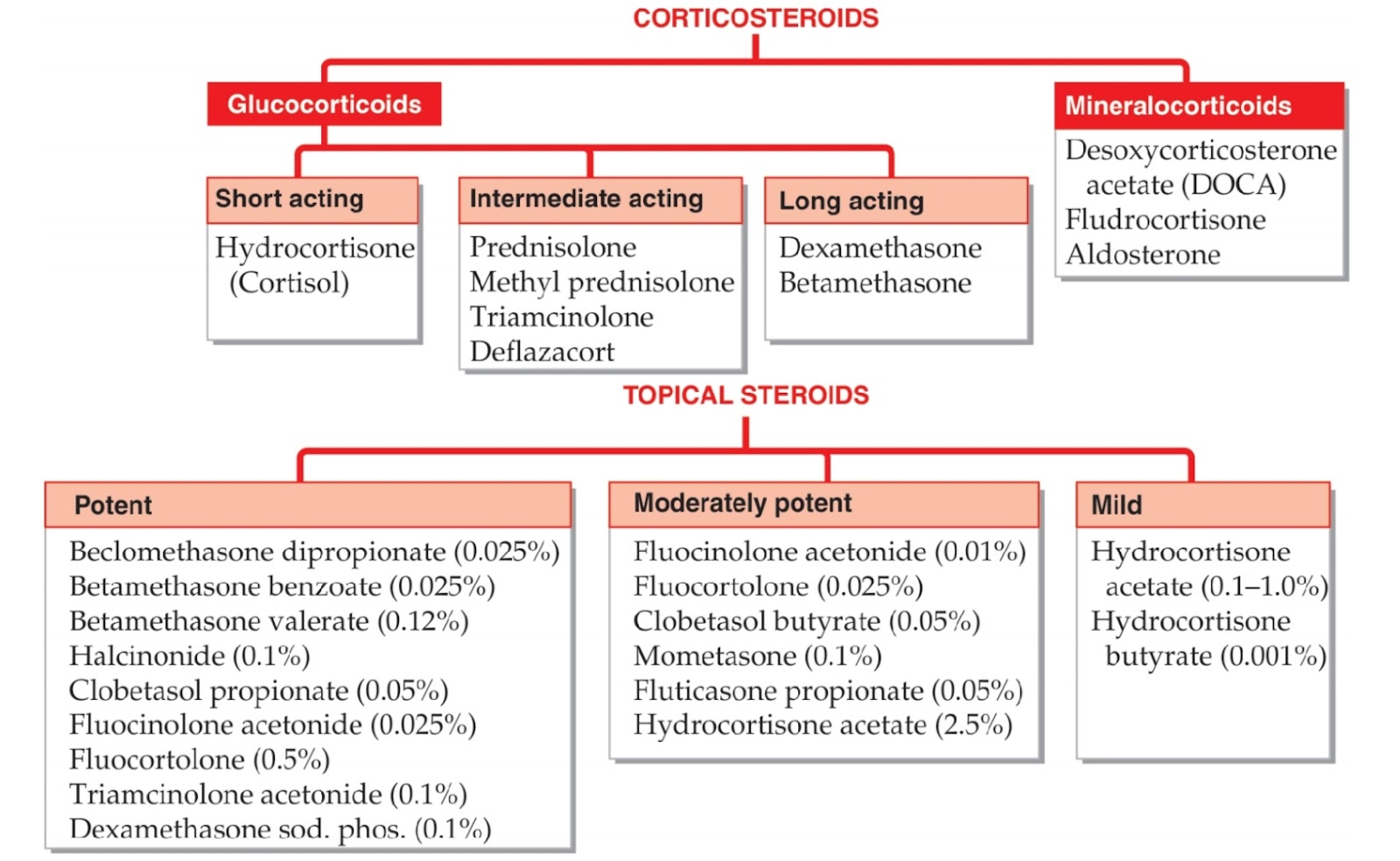
Mineralocorticoids
Major endogenous mineralocorticoid: aldosterone.
It acts on DCT of the kidney to cause reabsorption of Na+ and excretion of K+ and H+ ions.
It also is also involved in causing myocardial remodeling associated with CHF and the drugs blocking this effect [spironolactone, ACE inhibitors, angiotensin receptor antagonists and β blockers] decrease the mortality in patients with CHF.
Excess of mineralocorticoids causes sodium and water retention leading to hypertension and edema, hypokalemia and alkalosis.
Reduced mineralocorticoids can lead to Hypotension, hyperkalemia and acidosis.
Glucocorticoids
Major endogenous glucocorticoid: hydrocortisone.
On metabolism:
These are catabolic in nature.
They cause breakdown of carbohydrates (hyperglycemia), proteins (muscle wasting) and fats.
They causes redistribution of fat: deposition of fat on neck (moon face), around mouth (fish mouth), and back (buffalo hump) and removing the fat from extremities.
They decrease the intestinal absorption of calcium, enhance renal excretion, bone resorption leading to negative calcium balance and osteoporosis.
On GIT:
It increases the GI secretion(HCl, pepsin) and can aggravate peptic ulcer.
On CVS, CNS:
They prevent the increase in the permeability of capillaries.
These have mild euphoric effect and high doses can lower seizure threshold.
On blood:
Destruction of T cells and B cells in malignancies.
Sequestration of lymphocytes, eosinophils, monocytes and basophils in tissues - decrease in the circulation.
But, circulating neutrophils are increased due to release from bone marrow.
On immunity:
They suppress cell mediated immunity more than humoral immunity.
They inhibit the recruitment of immune cells.
They inhibit the release of IL-1 and IL-2.
On inflammation:
Powerful antiinflammatory agents
They inhibit chemotaxis.
They induce production of Annexin. It inhibits phospholipase A2 production.
They also delay wound healing and scar formation.
Uses of Corticosteroids
Replacement therapy:
Acute adrenal insufficiency - i.v. hydrocortisone.
Chronic adrenal insufficiency (Addison’s disease) - oral hydrocortisone and fludrocortisone.
Congenital adrenal hyperplasia (CAH)
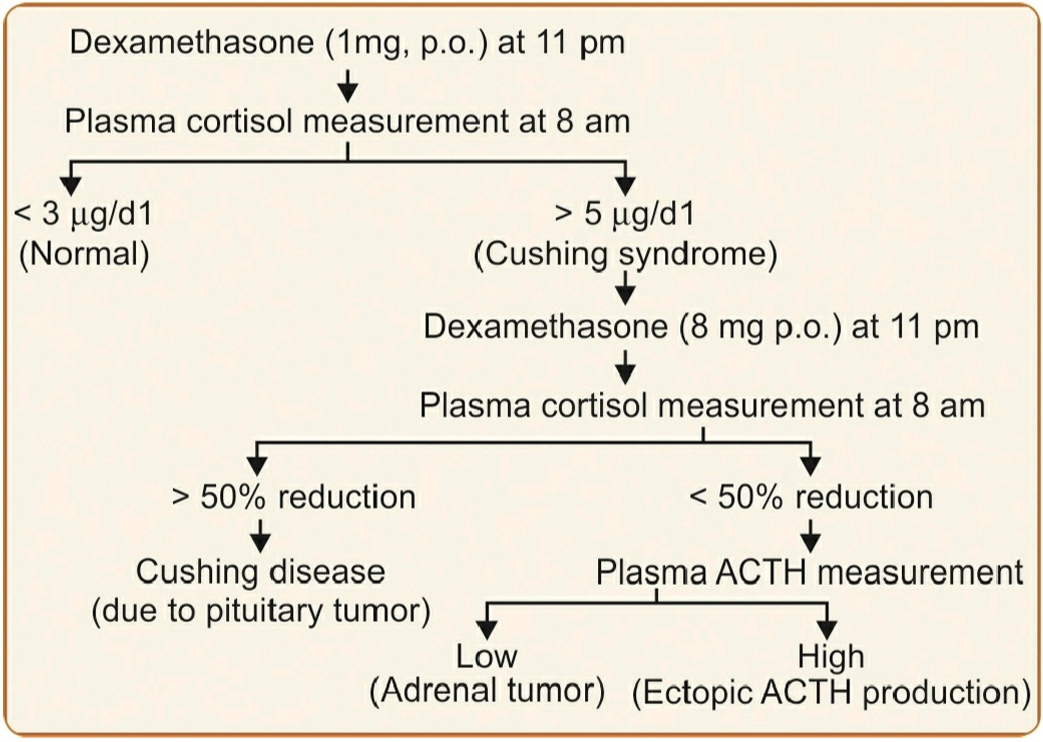
Diagnostic use:
Dexamethasone suppression test - to assess HPA axis.
Antenatal use:
Betamethasone accelerates the fetal lung maturation, if delivery is anticipated before 32 weeks of gestation.
Antenatal steroids may decrease the incidence of respiratory distress syndrome, PDA, necrotizing enterocolitis and periventricular/intraventricular hemorrhage.
As betamethasone is not available in India, dexamethasone is used.
Dexamethasone - 6 mg 12 hourly for 4 doses
Betamethasone - 12 mg 24 hourly for 2 doses
Non adrenal uses:
Anti inflammatory: used in rheumatoid arthritis, osteoarthritis, acute gouty arthritis.
Anti- allergic: for anaphylactic shock, urticaria, angioedema and serum sickness, chronic asthma.
Skin conditions like pemphigus vulgaris, exfoliative dermatitis and Steven Johnson syndrome also require systemic steroid therapy.
Immunosuppressive: High dose corticosteroid therapy is required in the organ transplantation to prevent graft rejection. It is used in autoimmune diseases like myasthenia gravis, hemolytic anemia) and collagen vascular diseases (like SLE, polyarteritis nodosa and nephrotic syndrome). Steroids are also used in ulcerative colitis and Crohn’s disease.
Anti-cancer: used in Hodgkin’s and non Hodgkin's lymphoma, ALL, CLL, multiple myeloma, Carcinoma breast. These can also be used with anti-neoplastic agents to decrease nausea and vomiting.
Deflazacort - in Duchenne muscular dystrophy
Corticosteroids with selective glucocorticoid action(dexamethasone , betamethasone) - to decrease cerebral edema
Can be used in septic shock
Can be used in sarcoidosis
Prednisolone is used to decrease bleeding tendency in thrombocytopenia.
Autoimmune hemolytic anemia is treated with prednisolone.
Significant decrease in neurological defects have been seen in spinal cord injury patients treated with large doses of methylprednisolone (within 8 hours).
Prednisolone produces dramatic relief in eosinophilic pulmonary syndromes like Loeffler syndrome.
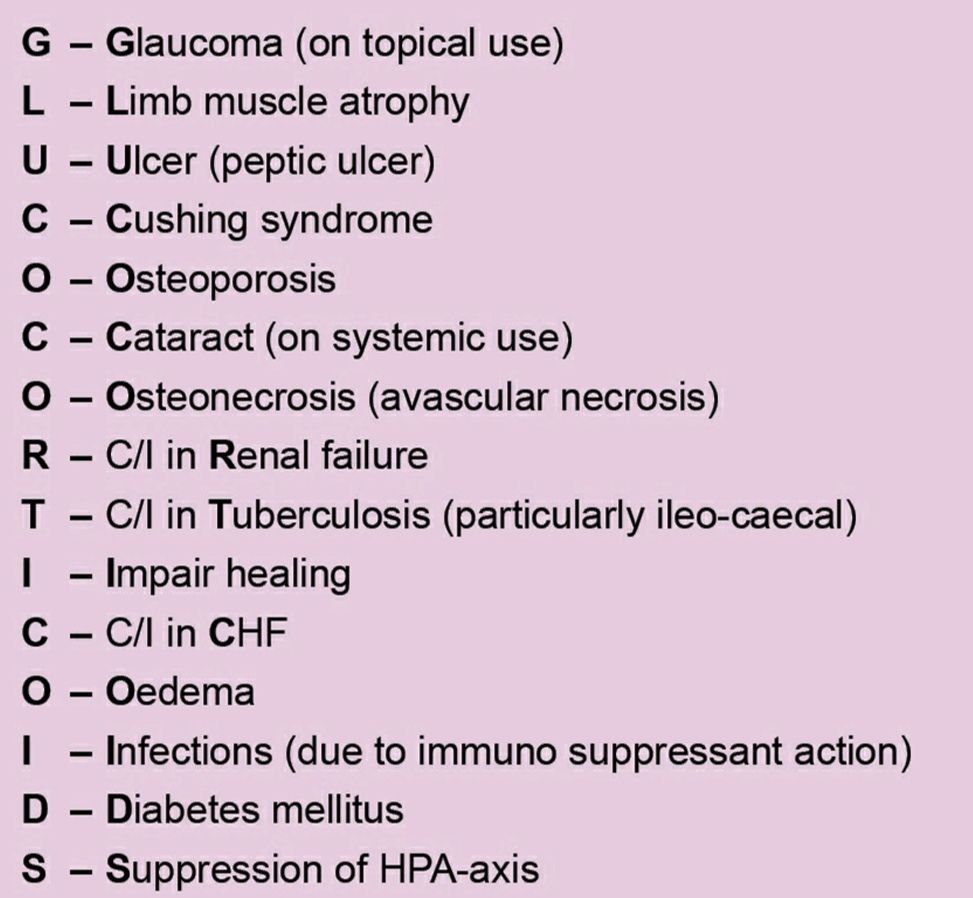
Adverse effects and contraindications
Hypertension
Hypokalemia
Alkalosis
Edema
Hyperglycemia
Osteoporosis
Cushing habitus
Posterior subcapsular cataract ( on systemic use)
Glaucoma (on topical use)
Increased susceptibility to infections - due to immunosuppressive action
Delayed wound healing
Osteonecrosis especially in hips
Contraindicated in psychosis, peptic ulcers, etc.
Caution
Long term use (more than 2 weeks) of Corticosteroids can cause suppression of the HPA axis.
To prevent HPA axis suppression, steroids can be given on alternate days but long acting steroids like betamethasone and dexamethasone cause HPA axis suppression even when administered on alternate days.
Steroids should not be withdrawn abruptly because it may precipitate acute adrenal insufficiency. Tapering of steroids is very important.
Large single doses are less harmful than small doses given for long periods.
A patient on steroids, during any stressful conditions like trauma, surgery - dosage should be increased (2-10 folds). Do not reduce the steroid dosage.
Reference:
Essentials of Pharmacology by K D Tripathi
Review of pharmacology by Sparsh Gupta
1 comment