
Angioedema
Introduction
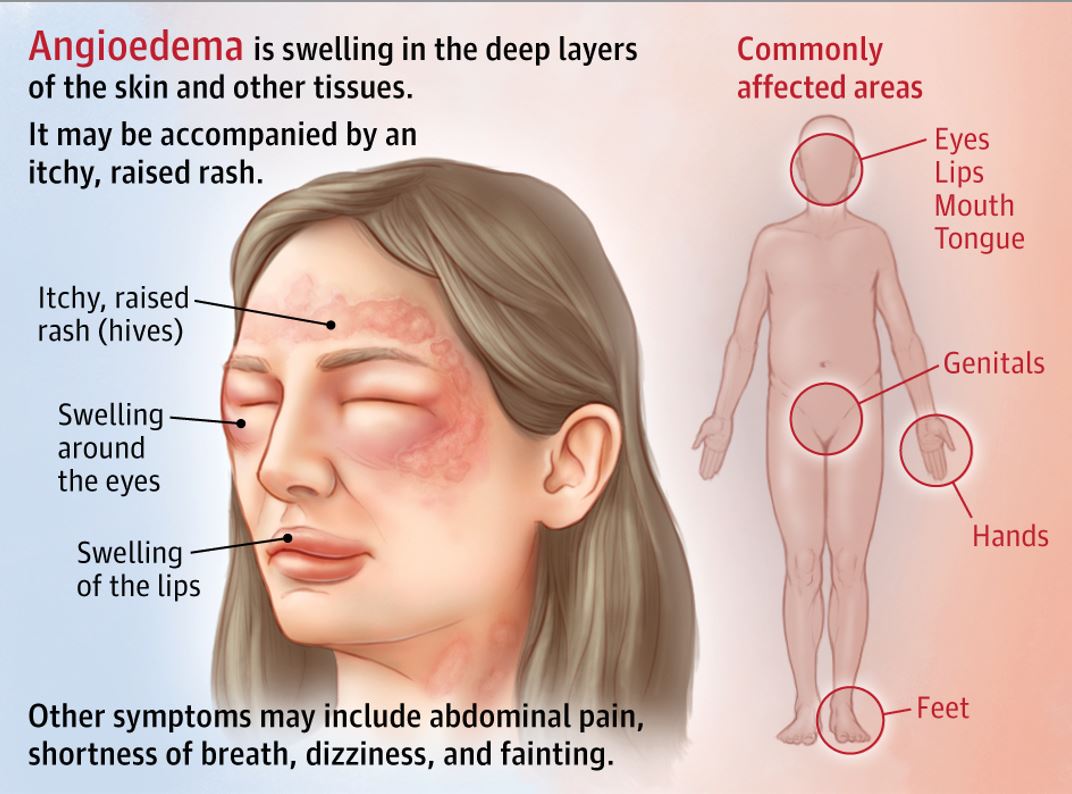
Angioedema can be defined as subcutaneous tissues and/or submucosal tissues circumscribed non-pitting edema affecting lips, face, neck, extremities, oral cavity, larynx, and gut.
It is self limiting and localised swelling resulting from extravasation of fluids into interstitium due to the loss of vascular integrity.
It becomes life-threatening when it involves the larynx causing respiratory obstruction, while intestinal angioedema is painful.
Etiology
Inherited - hereditary angioedema:
Due to mutation in general encoding for C1 inhibitor molecules. It follows an autosomal dominant inheritance pattern.
C1 inhibitor is a serine protease inhibitor (SERPIN). C1 inhibitor deficiency is associated with SERPING 1 mutation or mutated genes which encode for metabolizing and functioning enzymes of bradykinin.
Acquired causes:
It includes lymphoproliferative disorders, autoimmune disorders, neoplasms, infections, and drug induced.
Classification
Idiopathic
Medication induced
Allergen induced
Physically induced
Due to deficiency of C1 esterase inhibitor
Hereditary angioedema (HAE) with C1 INH deficiency
Type 1 - lack of C1 esterase inhibitor molecule
Type 2 - dysfunctional C1 esterase inhibitor molecule
Acquired angioedema (AAE) with C1 INH deficiency
Variant 1 AAE - associated mainly with lymphoproliferative disorders
Variant 2 AAE - anti C1 INH autoantibodies
Angioedema can also be classified into
Histamine mediated angioedema
Bradykinin mediated angioedema
Pathophysiology
Histamine-mediated angioedema is the most common and is secondary to mast-cells and basophil activation.
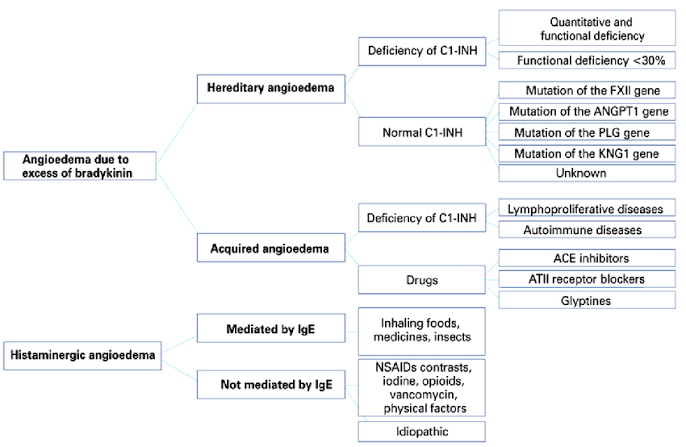
Bradykinin mediated angioedema:
Hereditary angioedema/ acquired C1 INH deficiency/ angiotensin converting enzyme inhibitor associated angioedema
It is not triggered by allergic reactions or hives.
C1-inhibitor is a regulator of complement and the contact system; if deficient or dysfunctional it causes activation of the contact system resulting in uncontrolled production of kallikrein leading to proteolysis of high-molecular-weight kininogen and bradykinin, leading to edema by increasing in vascular permeability.
C1 inhibitor deficiency: Excessive production of bradykinin
Angiotensin-converting enzyme inhibitor-associated angioedema: Decreased degradation of bradykinin
Histamine and bradykinin increase localized microvascular permeability.
NSAID induced: cyclooxygenase 1 inhibitor affects arachidonic acid metabolism, leukotriene/prostaglandin binding to the receptor or may be IgE mediated
Presentation
Histaminergic angioedema:
Skin - urticaria, flushing, pruritus
Respiratory - bronchospasm
GI - abdominal pain, vomiting
Onset is within 60 minutes of allergen exposure; it may last for 1 to 2 days.
NSAID induced angioedema: urticaria and facial swelling.
Bradykinin mediated angioedema:
Not associated with urticaria
More severe and for longer duration
Associated with severe abdominal symptoms
Management
In all forms of angioedema, a key aspect in disease management is taking steps to lower the risk of future swelling attacks.
For few patients, preventing future angioedema attacks may include resorting to medications that are taken regularly to reduce the risk of swelling. In cases where angioedema is found or suspected to have been triggered by a medication, stopping that medication — and finding a suitable alternative — is key in preventing future swelling episodes.
In hereditary angioedema, swelling attacks may be triggered by physical injury, stress and infections. Thus, disease management often includes steps to minimize the chances of injuries or infections.
Histaminergic angioedema: antihistamines, corticosteroids, epinephrine(emergency management)
Hereditary angioedema attacks should be treated with C1 Inhibitor concentrate, ecallantide (Kallikrein inhibitor) or icatibant (bradykinin-receptor antagonist).
Acquired angioedema related to angiotensin-converting enzyme (ACE) inhibitor is treated with antihistamines, epinephrine, and glucocorticoids.
Post a Comment