
Magnets in Orthodontics
Introduction
Magnet is a material that is capable of producing magnetic fields and is capable of attracting ferromagnetic materials like iron, nickel and cobalt. Magnets are classified into permanent, temporary and electromagnets.
For more than 2 decades, magnets have been used in the medical and dental field for various purposes. The increase in use of magnets is due to the availability of smaller, powerful permanent magnets. In dentistry, various rare earth magnets are used in the prosthodontics and orthodontics field for denture fixation and as force systems in tooth movements respectively.
Static magnetic fields are produced by magnets used in orthodontics. The WHO report of 1987 states that static magnetic fields up to 2T show no significant health effects.
Magnetic materials used in dentistry are as follows:
Platinum-Cobalt (Pt-Co)
Ferrite
Neodymium-iron-boron (Nd-Fe-B)
Chromium-cobalt-iron (Cr-Co-Fe)
Samarium-cobalt (Sm-Co)
Aluminum-nickel-cobalt (Al-Ni-Co)
Classification of magnets used in dentistry
Based on alloys used
Cobalt containing, e.g. Alnico, Alnico V, Co- Pt, Co5Sm
Non-Cobalt containing, e.g. Nd-Fe-B, samarium iron nitride
Based on ability to retain magnetic properties:
Soft - easy to magnetize or demagnetize and less permanent. Example: Pd-Co-Ni alloy, Pd-Co alloy, Pd-Co- Cr alloy, Pd, Co-Pt alloy, magnetic stainless steels.
Hard - retain magnetism permanently. Example: Alnico alloys, Co-Pt, Co5Sm, Nd-FeB.
Based on type of magnetic field:
Open field
Closed field
Based on the type of magnetism:
Repulsion
Attraction
Based on surface coating:
Surface coating materials - stainless steel, titanium or palladium
Coated
Uncoated
Based on the arrangement of the poles:
Reversed poles
Nonreversed poles
Based on number of magnets in the system:
Single
Paired
Applications in Orthodontics
The use of magnets for orthodontic tooth movement was first described by Blechman and Smiley in1978. The various applications of magnets in orthodontics are listed below.
Simple tooth movement without archwires
Relocation of Unerupted teeth
Space closure with magnets
Molar intrusion and correction of anterior open bite
Molar distalization
Maxillary expansion
Functional appliances for correction of Class II malocclusion
Functional Appliances for Class III malocclusions
Treatment of obstructive sleep apnea, snoring
Extrusion of crown-root fractured teeth
Lingual retainer
Simple tooth movement without archwires:
Muller suggested the use of small SmCo magnets (approximately 531 mm) to deliver light continuous forces to close diastemas without archwires. He prescribed magnet size of 5mm×3mm×1mm. To the labial aspect of the teeth magnets were bonded. For better control of the tooth, a mesial slant is given for the two magnets. The rotations can also be corrected with magnets.

Relocation of Unerupted teeth:
Two attracting magnets can be used to move the impacted tooth. One magnet is bonded to the impacted tooth and the other stationary magnet is placed outside in a removable acrylic plate. The activation is done by repositioning of the magnet within the plate.
Space closure with magnets:
A soldered Sm-Co magnets plated with nickel and chromium to Edgewise brackets can be used to deliver mesio-distal magnetic forces. This can be used to close the extraction spaces. It decreases the treatment time.
Molar intrusion:
The magnetic force can be used in conjunction with a corticotomy procedure, to intrude over erupted molars following loss of their antagonist. Bite-block appliances containing magnets enhance the intrusion of buccal segments in cases with anterior open bite.
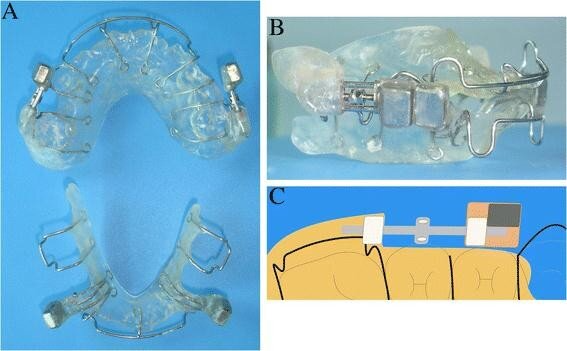
Molar distalization:
intra-arch placement of repelling magnets against the maxillary molars along with a modified Nance appliance cemented on the first premolars, can be used to distalize the Class II molars - Gianelly et al. Molar Distalization System by Itoh et al uses repelling magnets to cause molar distalization. The mesial magnet of each pair is mounted so that it can move along a sectional wire.
Maxillary expansion:
Vardimon et al investigated the impacts of magnets to give extension drive in monkeys and presumed that:
Magnetic apparatuses were found to convey constrain in superolateral bearing.
Overjet expanded because of extending transverse and sharp sutures.
Effects were more in molar regions.
Advantages in the use of magnetic forces are a predetermined force range with upper and lower limits eliminating the iatrogenic disturbances.
Functional Appliances:
For class 2 correction, FOMA II is introduced by Vardimon et al. Functional Orthopedic Magnetic Appliance II uses attracting upper and lower neodymium- iron-boron magnets to maintain the mandible in an advanced sagittal position.
Clinically, first class 2 correction was done by Magnetic Activator Device - MAD. Types of MAD include: lateral displacement (MAD I), class II malocclusions (MAD II), class III malocclusion (MAD III), and open bite cases (MAD IV).

Magnetic Twin Blocks include incorporating magnets to occlusal slanted planes. Clark used magnets in his Twin block for Class II division 1 malocclusion with huge overjet, Mellow remaining class II, buccal fragment relationship, Gentle class II the division 1 malocclusion, Grown-ups with serious class II division 2 malocclusion and, stamped skeletal class III malocclusion.

Extrusion:
Bondemark et al described the use of magnets to extrude the teeth with subgingival crown-root fracture in which the fracture line is difficult to access.
Lingual retainer:
Small magnets can be bonded in the lingual surface of lower anteriors without interfering with the tongue in post orthodontic treatment patients to act as a lingual retainer.
Tradename: Magnetainer


Advantages of using magnetic force in orthodontics
Consistent power - no power rot after some time
Better directional power
Subsequently magnets for intermaxillary footing don't have undesirable symptoms as class II class III elastics have.
Better power and working reach control - by keeping up the separation between magnets, better power level can be controlled.
Quick tooth development along these lines has less treatment length
Least apparatus alteration
Less seat side time
Disadvantages of using magnetic force in orthodontics
Corrosion of the magnets
Bulkiness of the magnets
Thermal affectability of magnets
Difficult to configure fitting size of magnets as they are hard and fragile in nature.
Post a Comment